Welcome to another edition of Back to the Basics! This time around, I thought I’d discuss chest trauma. The reason being, injuries to this part of the body are the second most common traumatic injury, and come with the highest cases of patient mortality; in some studies, up to sixty percent.5 You know very well that the chest contains many vital organs, blood vessels, and portions of the airway. As protected as these structures are with the ribs, laterally, the sternum, anteriorly, and the spine, posteriorly, nonetheless, blunt and penetrating chest injuries can catastrophically compromise a patient.

But, why? The answer is simple. Each injury, in its own way, negatively affects the body’s ability to ventilate, exchange oxygen and carbon dioxide, and/or sustain adequate perfusion. As discussed in previous articles, if any of those components are compromised, it is harmful, and potentially, fatal. A flail chest, tension pneumothorax, cardiac tamponade, and pulmonary contusion all have unique presentations, but in the end, their presence jeopardizes any of the aforementioned vital functions. Let us take a closer look…
Flail chest
Flail chest presents with at least two fractures of at least three consecutive ribs, typically caused by blunt injuries to the anterior or lateral thorax. The affected area loses connection with the surrounding bone structure, and in many instances, the injury only reveals itself during palpation of the chest. Instability between the fractured rib segments, along with the associated crepitus, makes its presence obvious to the EMS professional. If observed during the physical exam, the telltale flail chest sign is paradoxical movement. The fractured segment appears to suck inward during inspiration (chest should expand) and pop out during expiration (chest should collapse). However, if a patient is obese, has a large amount of breast tissue, or the segment is relatively small, this sign can get missed.
Many trauma-scoring systems consider a flail chest as one of the most serious cases, with a mortality rate reaching upwards of 40%1 and having profound adverse effects on ventilation. First and foremost, rib fractures HURT! Any chest expansion past a certain point rubs the broken bone ends together, creating excruciating pain. As a result, a patient’s natural tendency is to take shallower-than-normal breaths, called “splinting.” Tidal volume subsequently diminishes, compromising the ventilatory process. Also, recall the connection between the visceral and parietal pleura, with glue-like pleural fluid between these two layers.
When the intercostal muscles contract and expand the chest, the parietal layer pulls the visceral layer along with it, subsequently expanding the entire lung. This action decreases intrathoracic pressure and helps achieve adequate inspiration. However, at the site of injury, this action is lost, as the area of the lung under the flail segment does not move with the chest during inspiration. If the flail segment is large enough, the remainder of the intact rib cage cannot expand enough lung mass to produce an adequate inspiration. The total inspiratory volume becomes less and less, and proper oxygenation and carbon dioxide elimination cannot take place. Management of a flail chest, thus, centers on maintaining an airway, adequate oxygenation by the most appropriate means, assisted ventilation with BVM as needed, and pain control.
Tension Pneumothorax
A pneumothorax develops because free air enters the chest. Often resulting from blunt trauma, consequently rupturing one or both lungs, which then leak air into a closed, intact chest. The other mechanism involves a hole (usually from a gunshot or stabbing) that allows air to move from outside of the body through that opening, then directly into the chest cavity.
Air invades the pleural space and starts to expand between the two layers. At some point, the pleural fluid loses its tension, and the connection between the lung and the thorax severs. This happens in a relatively short period, typically within a few ventilations. Why, you ask? Reason one, the patient is injured and in pain. Ventilatory rate naturally increases, which then accelerates air entry into the chest—reason two, simple chemistry. When you place a gas into an environment and warm it rapidly, it expands. Therefore, except for the odd, obnoxiously hot and humid summer day, ambient air temperature is not the body’s normal 98.6o. When that “colder” external air enters the chest from an open wound, it rapidly expands within the “hotter” chamber/pleural space. Unchecked, air increasingly enters the chest, the pleurae eventually separate, and the affected lung loses expansion and contraction ability.
The ensuing lung compression collapses the lower airway passages and alveoli, cutting off airflow to the pulmonary circulation. At this point, decreased/diminished lung sounds (and eventual lack, thereof) are auscultated, unequal chest rise and fall are observed, and hyper resonance is percussed (a hollow thoracic sound due to the overwhelming presence of air). The patient increases the rate of breathing with shallower breaths and develops a feeling of severe breathlessness, known as air hunger. The progressive hypoxemia eventually causes agitation, apprehension, and cyanosis. Free air within the thorax may also leak into the surrounding skin layers, especially as the internal thoracic pressure increases. This is called subcutaneous emphysema and has the consistency of bubble-wrap when palpated. However, as tempting as it may be, DO NOT try to pop the bubbles!!
Once the thoracic pressure is high enough, the expanding air pocket shifts the heart and other mediastinum structures toward the opposite side of the chest. A perfusion problem develops as the heart compresses the vena cava, cutting off cardiac blood return. Cardiac output and blood pressure decrease, and jugular venous distention occur as blood is forced backward into the superior vena cava and external jugular veins. Signs of decompensated shock appear, and in a very rare and late instance, IF it is observed, the trachea deviates toward the uninjured side of the chest.
So, that being said, when the signs as mentioned earlier and symptoms materialize, the injury is no longer a “simple” pneumothorax, but rather, a tension pneumothorax. Prehospital management revolves around trying to correct the ventilation and the perfusion deficit. At the EMT level, attaining and maintaining good oxygenation (possibly with a BVM), covering an open chest wound with an occlusive dressing, treating for shock, and rapid transport to an intercepting paramedic or the closest, appropriate ED is imperative. Additionally, a paramedic may be able to buy the patient time by inserting a long (typically > 3 inches) and relatively wide (14 gauge or larger) into the anterior chest over the third rib, mid-clavicle. The alternative location is the mid-axillary or anterior axillary line, into the fourth intercostal space. Air rush may be heard, but regardless, the negative effects of the tension should begin resolving within a short time if the catheter is placed correctly.
Cardiac Tamponade
This injury is one of least common, but also highly fatal. It occurs in less than 1% of patients with chest trauma and associated myocardial rupture2, but the mortality rate varies, ranging from 75% to 81%3. Here’s why. Recall the serous membrane surrounding the heart called the pericardium. The visceral layer (the epicardium) covers the heart surface, and the parietal layer (made of fibrous tissue) encapsulates the entire organ. Between these layers is 10-50 ml of pericardial fluid, which acts as a lubricant, allowing the two layers to glide over each other with each heartbeat. When excessive volume fills the pericardial sac, the result is cardiac tamponade. Left unchecked, it decreases overall systemic perfusion.
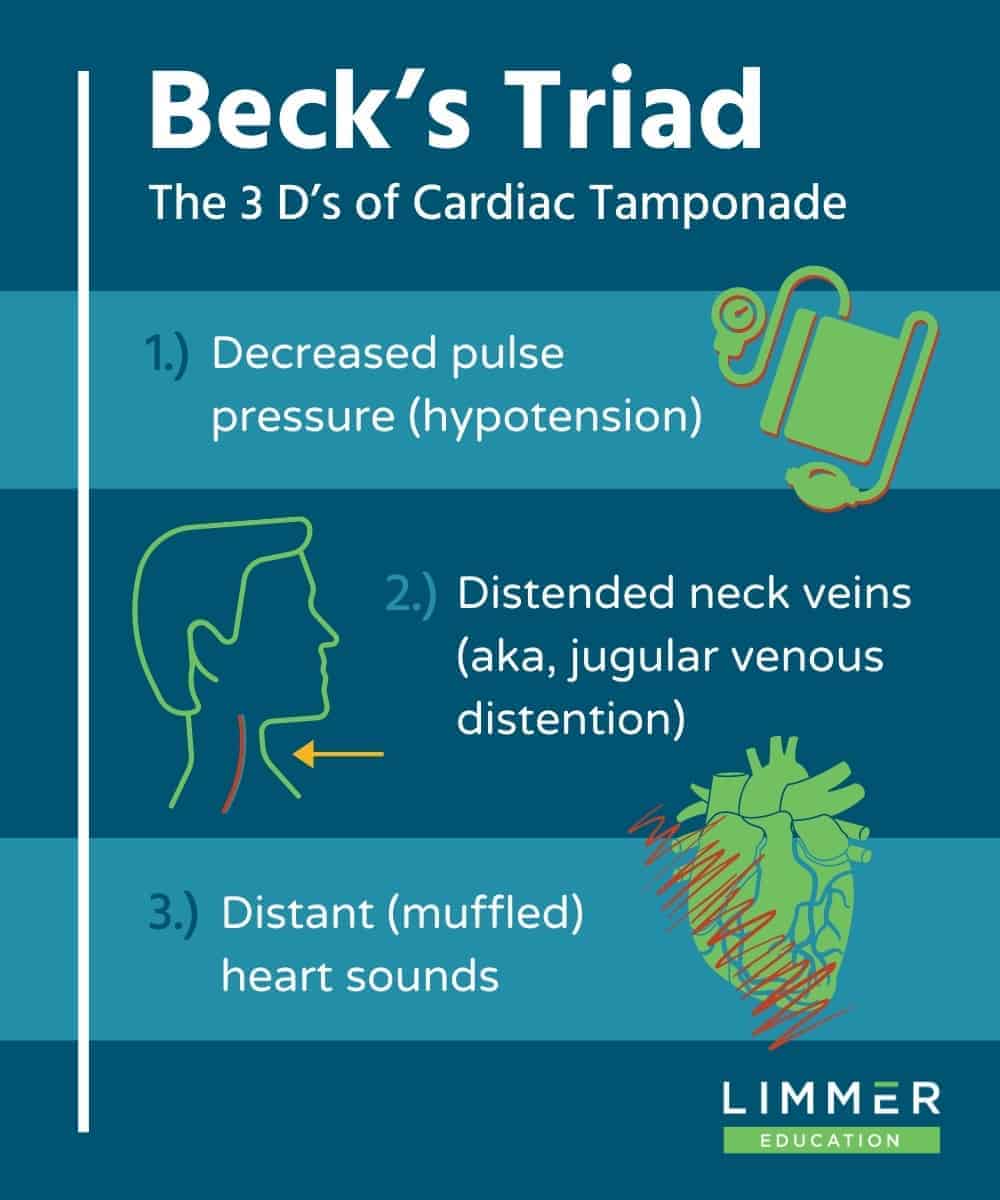
If the fluid accumulation is slow, the pericardial sac can expand to contain more than two liters. However, if it is rapid, as little as 200 mL can result in tamponade.4 In either regard, pressure continuously builds within the pericardial sac (just like slowly squeezing a stress ball). Eventually, the atria and ventricles lose their ability to fill and contract, and the patient becomes pulseless. Yet, before this happens, jugular venous distention, muffled heart sounds, and hypotension with a narrowing pulse pressure can be detected during a physical exam.
{kind=link}
Collectively known as Beck’s triad, these signs only occur simultaneously during cardiac tamponade. Jugular venous distention materializes when blood cannot passively flow through the increased intracardiac pressure. Ensuing retrograde blood flow increases venous pressure within the superior and inferior vena cavae and, eventually, the external jugular veins. Pearl of Wisdom: only cardiac tamponade and tension pneumothorax produce jugular venous distention with a chest injury. How you tell the difference is by auscultating the lungs. Tamponade will typically reveal clear, bilateral, lung sounds while a tension pneumothorax will not. The excessive blood surrounding the heart not only dampens audible heart sounds but also progressively reduces the hearts’ pumping strength and ventricular pressure (hypotension). The steady declining difference between the systolic and diastolic values reflects this (narrowing pulse pressure).
Prehospital management mostly revolves around a “recognize and run” approach. There is very little EMS professionals can do for a patient with tamponade, outside of maintaining adequate oxygenation, IV fluid support, and “diesel therapy”. If the patient arrests, standard BCLS and ACLS algorithms should be followed; the peri-arrest phase usually produces a PEA rhythm. The definitive stabilizing measure is removing the excess fluid from the pericardial sac, called a pericardiocentesis. Decreasing time in the field is essential, as only an ED physician can perform this procedure.
Pulmonary Contusion
Pulmonary contusion is a common consequence of blunt chest trauma, sometimes occurring in conjunction with a flail chest. It can also result from an explosive shockwave injury or from cavitation forces generated when a high-velocity projectile, such as a bullet, travels through the lung. Children especially are at high risk due to the relative flexibility of their rib cage. Their chest wall poorly absorbs an impact, allowing greater force transmission into the lung. Regardless of the mechanism, capillaries are ruptured, which then bleed into lung tissue, and eventually, the alveoli.
Remember, respiration requires very close proximity between alveoli and pulmonary capillaries (the respiratory membrane). As blood accumulates within the respiratory membrane, it widens that distance, markedly delaying the exchange of oxygen and carbon dioxide. Likewise, gas does not move through liquid very efficiently, nor quickly. Now, not only is blood present in the respiratory membrane, but eventually, it leaks into the alveoli, causing it to fill with proteins (the inflammatory response) and then collapse – further widening the respiratory membrane. Consequently, the bigger the contusion, the less the lung can effectively exchange carbon dioxide and oxygen.
This condition can take minutes or hours to develop, and as such, may rarely show any signs and symptoms during prehospital care. However, there is always the possibility of long transport time, an initial delay discovering the victim or a prolonged entrapment/extrication time. These patients likely will present markedly hypoxemic, pale/cyanotic, and in respiratory distress. Decreased breath sounds and rales may be auscultated over the contused area. The patient may also be wheezing and/or coughing up watery, blood-tinged sputum. Management necessitates high-flow oxygen administration, assisted ventilation, and/or intubation. Examine the patient for any other associated injuries and transport immediately.
Ventilation, respiration, and perfusion are processes vital to maintaining life, and traumatic chest injuries can disrupt one, two, or all three in an instant. I gave you four examples of how this happens, but be aware there are many others. Contusions to the heart, rupture of major blood vessels, and tears of the trachea and diaphragm are just a few. Whatever the mechanism may be, keep in mind that any chest injury, can, and will, breach the natural order and compromise your patient. Your rapid recognition and stabilization may very well save their life.
References
1. Engel C, Krieg J C, Madey S M, Long W B, Bottlang M. Operative chest wall fixation with osteosynthesis plates. J Trauma. 2005;58(1):181–186.
2. Martin TD, Flynn TC, Rowlands BJ, Ward RE, Fischer RP. Blunt cardiac rupture. J Trauma. 1984;24(4):287-90.
3. Fulda G, Brathwaite CE, Rodriguez A, Turney SZ, Dunham CM, Cowley RA. Blunt traumatic rupture of the heart and pericardium: a ten-year experience (1979-1989). J Trauma. 1991;31(2):167-72.
4. Richardson, L (November 2014). Cardiac tamponade. Journal of the American Academy of Physician Assistants. 27 (11): 50–1.
5. Clark GC, Schecter WP, Trunkey DD. Variables affecting outcome in blunt chest trauma: flail chest vs. pulmonary contusion. J Trauma. 1988 Mar;28(3):298-304.